Naltrexone is a non-opioid FDA-approved medication used to treat opioid use disorder and alcohol use disorder.
Naltrexone lowers your sensitivity and tolerance to opioids, potentially increasing your risk of overdose.
You can begin taking it once all opioids are out of your system.
Naltrexone is available as a daily oral pill or a monthly injection.
Medication can be life-changing while coping with an addiction. Currently, there are three FDA-approved Medications for Opioid Use Disorder (MOUD): buprenorphine, methadone, and naltrexone. Like the other two, naltrexone is prescribed to support your treatment and help prevent return-to-use. But unlike its fellow medications, naltrexone is a non-opioid and is also approved for treating alcohol use disorder.
This versatile medication can be a great option on your recovery journey, but like any medication, naltrexone has its pros and cons. There’s the fact that it can reduce alcohol and opioid cravings, but also there’s the element of having to wait at least a week after using opioids to start it.
“Some people choose it because it does not create physical dependence and can support abstinence and mental clarity,” says Danielle Bellosi, a peer recovery supervisor at Boulder Care.
With that said, we want you to understand the benefits and risks of naltrexone as clearly as you can. Here’s what you need to know.
A note on language
Sometimes the process of taking medications for opioid use disorder is referred to as medication-assisted treatment (MAT), but that term is considered to be outdated by most medical professionals, so we’ll be using “Medications for Opioid Use Disorder or MOUD instead.
Our program is based on your goals, not our rules.
Whether you want to reduce use or stop altogether, your care team has your back.
Naltrexone is a medication approved by the Food and Drug Administration (FDA) for treating opioid use disorder and alcohol use disorder. It’s an opioid antagonist that can block the pleasurable effects of alcohol and opioids.
Critically, unlike its fellow FDA-approved Medications for Opioid Use Disorder (MOUD), buprenorphine and methadone, naltrexone doesn’t reduce withdrawal effects. Instead, it only dulls the impact of actual opioids.
We’ll explain this further, but it’s important to point out right away that after taking naltrexone, your body will become re-sensitized to the effects of opioids. In other words, you won’t have the tolerance you might have had before. In certain cases, taking naltrexone while using opioids can increase your risk of overdose and death. That’s part of the reason your doctor will have you start naltrexone after opioids are completely out of your system.
When taken correctly, naltrexone can be an incredible part of your treatment. “For opioid use disorder, naltrexone is a relapse-prevention tool,” says Dr. Patricia Pechter, DABFM, a clinical quality improvement physician at Boulder Care.
The same is true if you use naltrexone to treat alcohol use disorder, but without the same overdose risks (no enhancement of alcohol’s sedative effects or respiratory depression).
How does naltrexone work in the brain?
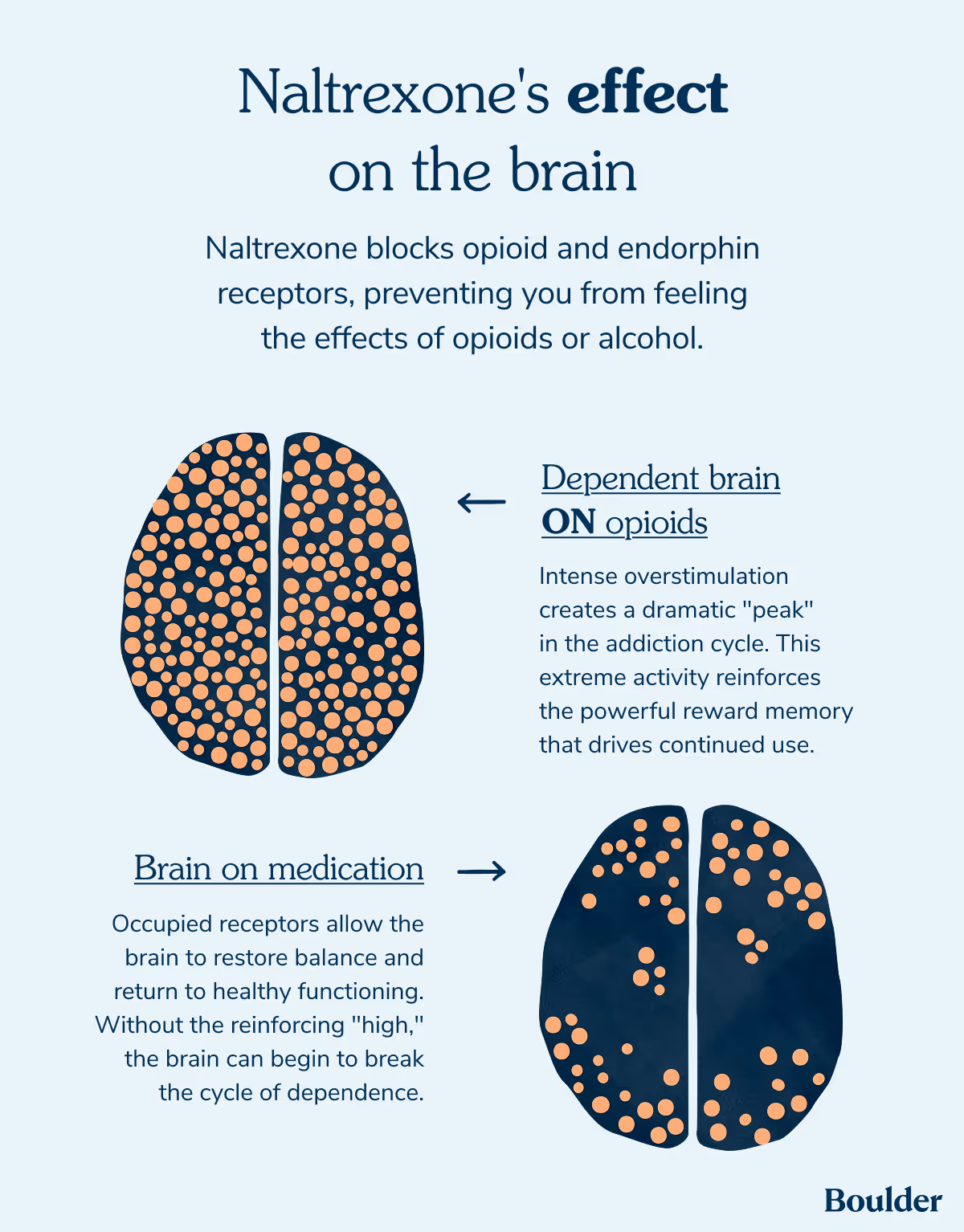
So, how does naltrexone work? Naltrexone’s role is reducing your urge to use opioids or alcohol. It blocks opioid and endorphin receptors, preventing you from feeling the effects of these substances. “Think of those receptors as parking spots. Opioids ‘park’ there to create pain relief and euphoria. Naltrexone ropes off those spots, so opioids can’t get in,” says Dr. Pechter.
This blocking allows you to create space between yourself and the sensation opioids and alcohol bring.
Notably, naltrexone can also cause precipitated withdrawal if you take it too soon after opioid use. “If naltrexone is initiated before someone is fully opioid-free—typically seven to 10 days for short-acting opioids, longer for methadone—it can trigger an abrupt, severe withdrawal syndrome,” says Dr. Appa.
Get the medication you need, and the support you deserve.
We provide FDA-approved medications for alcohol and opioid addiction — and support services to help you stay on track and reach your recovery goals.
Naltrexone is FDA-approved for treating opioid addiction and alcohol use disorder as a daily pill in generic form, and as a monthly injection under the brand-name Vivitrol. The Vivitrol option is an extended-release injection, often referred to as a Long Acting Injectible (LAI).
Naltrexone for opioid use disorder
Vivitrol blocks opioid’s effects, ideally reducing a person’s desire to take them. It’s not designed to mimic the feeling of opioids or to help with withdrawal symptoms—both of which Buprenorphine and Methadone do.
Again, you can’t start naltrexone until all opioids are completely out of your system — at least seven to 10 days post-use. Sometimes, your healthcare provider will test to see if opioids are still in your system with the naloxone challenge or urine test.
Naltrexone for alcohol use disorder
In contrast, naltrexone is available for people living with alcohol addiction use disorder as both Vivitrol and an oral pill. In both cases, the medication works by reducing alcohol’s effect and your cravings for the drug, with treatment often recommended for at least 12 months, but can last as long as you need.
Despite its proven impact, naltrexone is not a common treatment option for people with an alcohol addiction. “Naltrexone is significantly underutilized for alcohol use disorder relative to its evidence base — it's often not offered at all, which is a missed opportunity,” says Dr. Appa.
You might start naltrexone while you’re still drinking or before all alcohol is out of your system. However, your clinician might wait until you’ve stopped taking alcohol if you have a serious risk of severe alcohol withdrawal.
Benefits of naltrexone for addiction treatment
Naltrexone comes with a range of benefits for both opioid and alcohol use disorders. For many people, one of the most notable might be that, unlike buprenorphine and methadone, it’s not an opioid. There’s “no stigma associated with being on ‘another opioid,’” says Dr. Appa.
When taken properly, naltrexone can be an incredible part of achieving your recovery goals.
Naltrexone treatment allows you to get support both physically and socially. In reducing opioid’s and alcohol’s effects, naltrexone provides support in staying off previously used substances. “Its role is maintenance and return to use prevention, working best once someone has stabilized, and ideally alongside behavioral health support,” says Dr. Appa.
Oral naltrexone vs. monthly injection
If your provider decides naltrexone is the right option for your treatment, the next step will be deciding between a daily pill or a monthly intramuscular injection.
There are quite a few differences between taking daily oral naltrexone and the monthly injection that will help you and your provider decide which is right for you.
Oral naltrexone
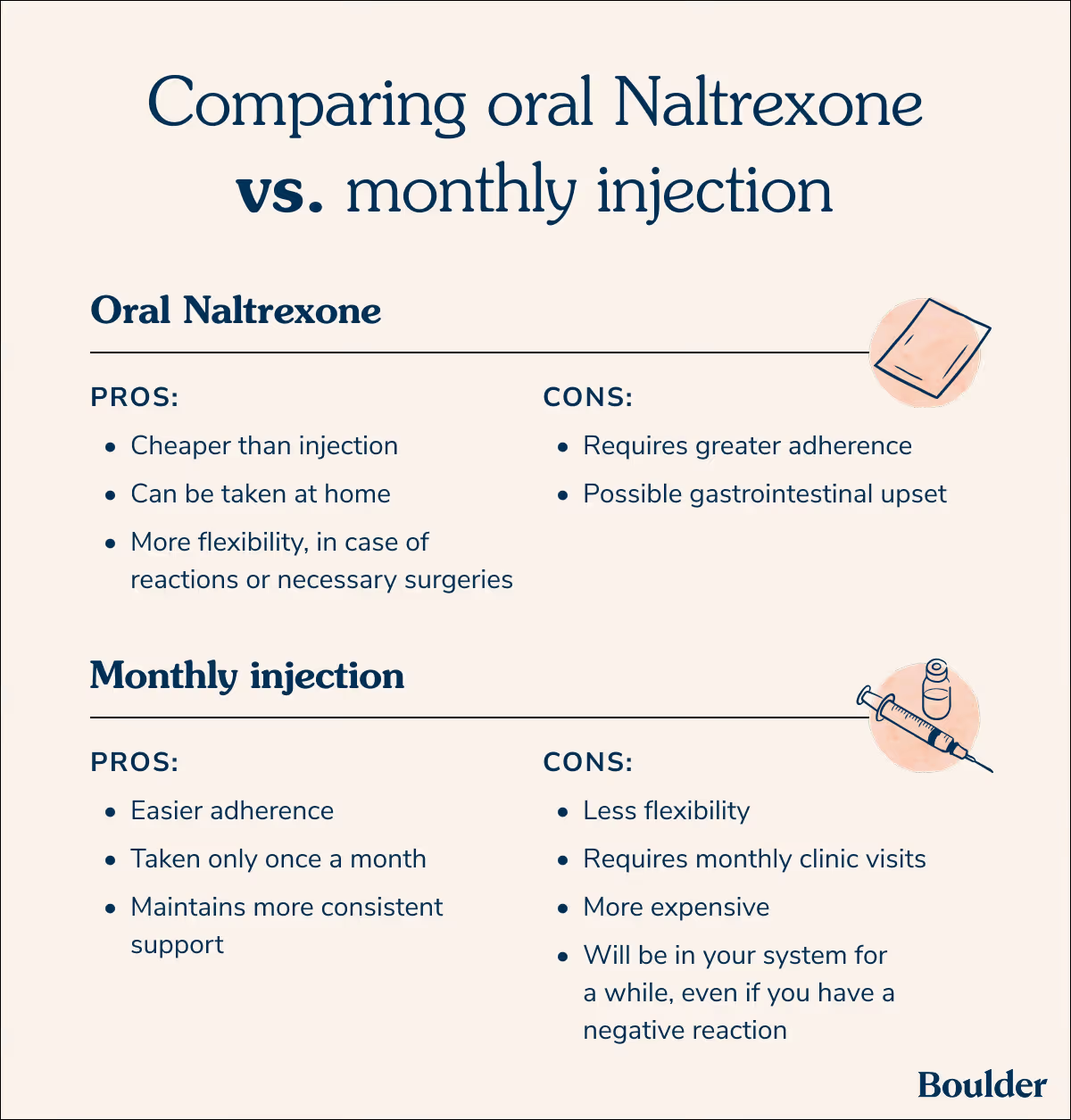
Oral naltrexone can feel like less of an ordeal since you can take it at home—it's also a lot cheaper than the injection. Plus, it offers you much more flexibility. For instance, if you had a sudden reaction to it or needed to stop taking it for a necessary surgery, you could do so immediately.
However, the at-home nature of oral naltrexone also means it requires much greater adherence—you have to take it consistently every day. So there's more control, but some people see it as a bigger commitment.
Flexibility can be important if you’re looking to get pregnant or need surgery. “For patients on naltrexone who need acute pain management—surgery or trauma—this requires careful planning,” says Dr. Appa. “Regional anesthesia, non-steroidal anti-inflammatory drugs (NSAIDs), and non-opioid adjuncts should be coordinated in advance, and oral naltrexone can be stopped 72 hours prior while injectable requires advance planning given its month-long duration.”
Oral naltrexone also has the potential to cause gastrointestinal upset.
Monthly injection
If you opt for the monthly injection of Vivitrol, you'll need to go to a clinic once a month for an intramuscular injection. This can sometimes be difficult if you don't live near a clinic that has it in stock. And if you have a reaction or need to get surgery, you can’t just stop taking it—the medication will stay in your system for a month.
However, one of the biggest advantages of the monthly injection is its easy adherence. You only have to take it once a month, meaning you don’t have to remember to take a pill every day. Plus, it can also provide you with more consistent support, maintaining strength throughout the month, as opposed to the pill, which weakens by the end of the 24 hours.
“From my own experience, Vivitrol offered a larger, more sustainable safety net while I worked toward stabilization, and I didn’t have to manage the daily decision of taking a pill,” Bellosi says.
What is low-dose naltrexone (LDN)?
There’s also the option of low-dose naltrexone (LDN). This is a pure inhibitor antagonist with absolutely no narcotic effect. It offers a dose that’s a tenth or less what a person normally gets of naltrexone. It can reduce pain and inflammation while increasing endorphin production.
Unlike recommended naltrexone doses for opioid use disorder and alcohol use disorder, much smaller naltrexone doses can help with a variety of conditions. There’s evidence of LDN helping patients with conditions such as Crohn’s disease, fibromyalgia, and multiple sclerosis, among others.
There’s also a chance of serious side effects while taking naltrexone. These side effects include:
Confusion
Hallucinations
Blurred vision
Elevated liver enzymes
Severe vomiting and/or diarrhea
The side effects of naltrexone will often go away as your body adjusts to the medication, but alert your healthcare provider if you experience any. Seek immediate medical attention if you experience any serious side effects or feel particularly unwell. Typically, you shouldn’t stop taking the medication without speaking to your medical provider.
Additional precautions and considerations
There are also certain precautions you might need to take before starting Naltrexone.
You should always tell your doctor about any medications you’re taking before starting Naltrexone because there are medications you can’t take at the same time.
Certain medications might cause a change in dosage or necessitate further monitoring.
While taking naltrexone, don’t start, stop, or change any other medications without consulting your doctor.
Before starting naltrexone, you should also let your doctor know if you currently have (or have ever had) depression or kidney disease. Naltrexone gets metabolized by the liver and is excreted from the kidneys, so if you’re living with kidney disease or liver issues it could require dosing adjustments.
Similarly, pregnancy and breastfeeding can be impacted if you’re prescribed naltrexone. Currently, there’s no clear understanding of Naltrexone’s safety during pregnancy.
Plus, you’ll need to alert all medical professionals that you are taking naltrexone before getting any sort of medical treatment or surgery, including dental surgery.
Naltrexone and opioid overdose risks
As mentioned before, naltrexone can reduce opioid tolerance and sensation, increasing your risk of an overdose. According to Dr. Pechter, risk is especially high at three times:
Near the end of a monthly injection cycle
After missing a dose
After stopping treatment
“In my experience, that blocking effect can reduce use — but it can also be dangerous if someone tries to override the medication by using more opioids,” says Bellosi. “Even if you don’t feel high, your body can still be affected, and overdose is still possible.”
With this in mind, Dr. Appa cautions, “Carry naloxone regardless.” Naloxone is an emergency injectable that can reverse the effect of an opioid overdose.
There are steps you can take to reduce your risk of opioid overdose while taking naltrexone. As Dr. Pechter explains:
Don’t skip doses
Don’t attempt to override the blockade with large opioid amounts
Work with a clinician on a clear safety plan, especially if stopping the medication
How to get naltrexone
Naltrexone is either available as an oral pill picked up from a pharmacy or by injection at a clinic site. Any provider licensed to prescribe medication should be able to write you a prescription for it.
It can’t be overstated that you must have all opioids out of your system before starting naltrexone.
Boulder Care has expert clinicians that can provide naltrexone prescriptions and tailored, ongoing treatment. We also provide telehealth, offering you greater flexibility as you navigate this time.
How much does naltrexone cost?
The cost of naltrexone is incredibly varied. To start off, how much is naltrexone without insurance? It might cost 30-something dollars for a 30 day supply, while one injection might be over $1,000. Your medical provider and local pharmacy can help you figure out exact costs and the cheapest option for you.
However, as of September 2024, Vivitrol claimed that using insurance or Medicaid allowed nine out of ten patients to pay less than $5 for the medication. There’s currently no generic version of Vivitrol approved, but it should also be available on cost-saving platforms like GoodRx.
Which is the better option for you: naltrexone or Suboxone
Naltrexone is one of three FDA-approved medications for opioid use disorder (MOUD), alongside buprenorphine and methadone. You and your provider will decide which option is best for you based on your medical needs and circumstances. Suboxone is the most commonly prescribed form of buprenorphine and is FDA-approved for opioid use disorder (OUD), but not alcohol use disorder (AUD).
"Neither medication is better than the other; they are used for different reasons," says Bellosi, who has taken both. Your provider can help determine which is the right fit.
Naltrexone
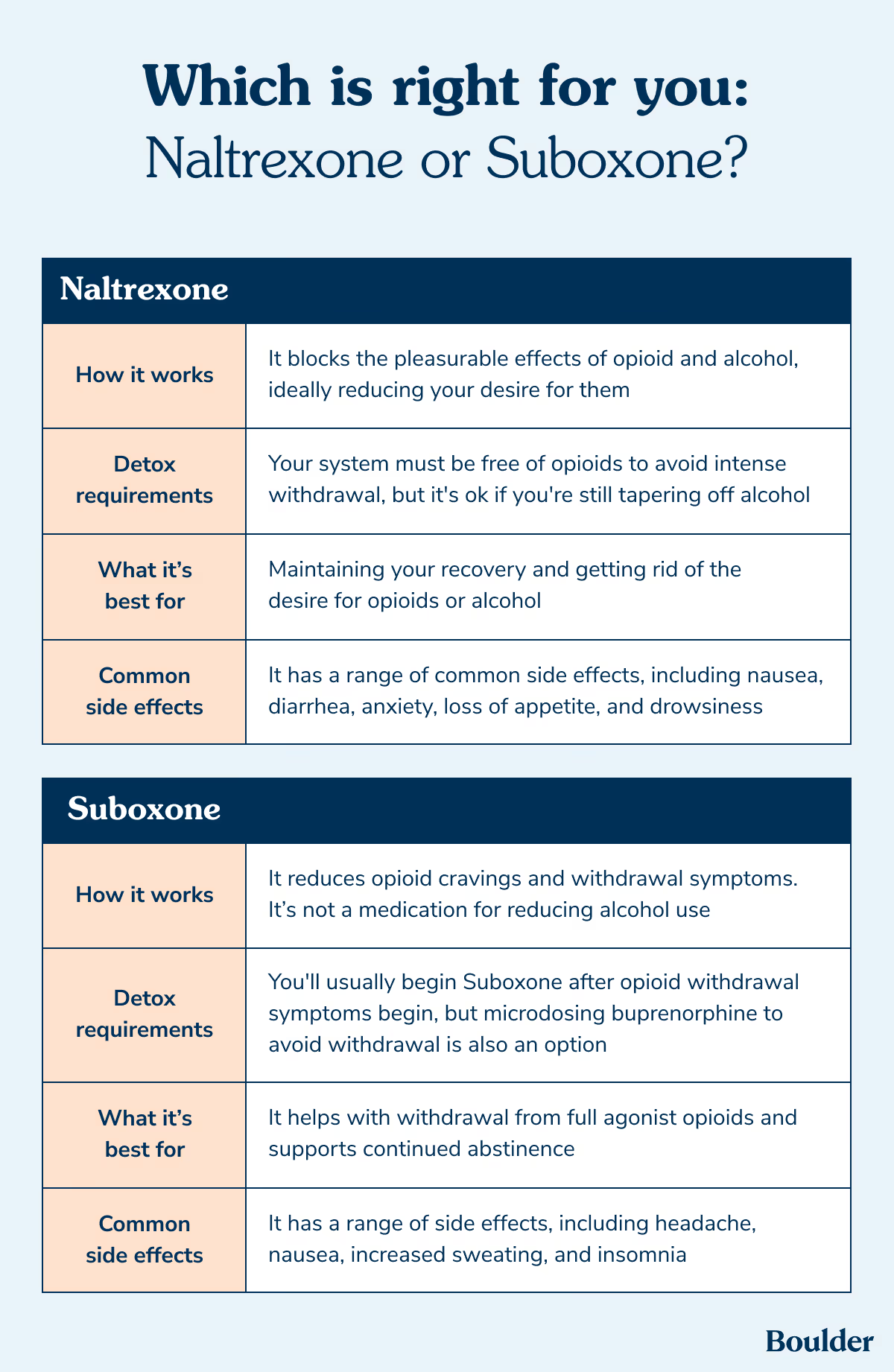
How it works: An opioid antagonist that blocks the effects of opioids and alcohol, ideally reducing your desire for them.
Detox requirements: Your system must be free from opioids before starting the medication.
Best for: Maintaining your recovery and getting rid of the desire for opioids or alcohol.
Common side effects: Some of the most common are nausea, diarrhea, anxiety, loss of appetite, and drowsiness.
Forms and dosing: Available as a daily oral pill, or a monthly injection as Vivitrol (administered at a clinicians office).
Suboxone (Buprenorphine)
How it works: Unlike naltrexone, Suboxone partially activates opioid receptors which eases withdrawal symptoms and reduces cravings. It's not used for alcohol use disorder.
Detox requirements: You should begin after opioid withdrawal symptoms appear — typically within 12 to 24 hours of last use. You will discuss timing with your doctor.
Best for: Managing withdrawal and sustained abstinence; a stronger option for patients at higher risk of return to use. Buprenorphine can also significantly lower overdose risk. "For someone transitioning from fentanyl or other opioids, buprenorphine or methadone are typically first-line because they reduce both cravings and overdose risk immediately," says Dr. Pechter.
Common side effects: Headache, nausea, increased sweating, and insomnia. Suboxone can also be used during pregnancy.
Forms and dosing: Typically taken once daily as a dissolving film or tablet, both available in generic form. Also available as weekly or monthly injections under the brand names Brixadi or Sublocade. Dosing requires care — too low a dose or tapering too quickly can trigger withdrawal.
What if you return to opiate or alcohol use while taking naltrexone?
You might return to use at some point and that’s nothing to be ashamed of. However, it’s important that you’re aware of the risk taking naltrexone can bring if you return to use. In the case of opioids, Naltrexone—and the time away from them—has left you with a lower tolerance and reduced sensitivity. This dangerous combination can provide an immense risk of overdose.
“When the brain’s opioid receptors are blocked for a while, the body may respond by making those receptors more sensitive or increasing their number,” says Dr. Pechter. “So if someone stops naltrexone and then uses opioids again, they can be much more vulnerable to overdose, even at doses they previously tolerated.”
Your risk is less severe if you take Naltrexone while consuming alcohol. Doing so might reduce your alcohol intake or urge to drink, but it’s still not advised to mix them. However, in both cases, you should immediately tell your provider so they can help you stay safe and possibly adjust the treatment plan if needed.
The bottom line
Naltrexone can be an incredible option as you navigate treatment for a substance use disorder, it just depends on what's right for you. “Naltrexone is neither ‘good’ nor ‘bad.’ It’s a tool,” says Dr. Pechter. “Tools work best when people understand how they function, and where the sharp edges are.”
Bellosi seconds this: “Both medication and recovery are deeply personal, and no two journeys look the same. Medication can be a helpful tool, not a moral statement. Stigma does not need to drive your decision-making. What matters most is what supports your health, safety, and quality of life.”
Our team at Boulder Care can provide you with guidance, support, and treatment for opioid and alcohol use disorder. Call 888-422-6530 to get started.
Frequently Asked Questions
What happens if I miss a dose?
Take your missed dose of naltrexone as soon as you remember it. However, if it’s close to the time you normally take naltrexone, instead skip the other dose and take your regular one. Don’t take two doses close together.
How do I get a naltrexone prescription?
Naltrexone is available as a prescription and any provider can prescribe the oral pill for you to pick up at your local pharmacy. The injection is available at clinics to be given by a medical professional.
Does naltrexone help with anxiety?
Studies have shown that off-label use of low-dose naltrexone (LDN) may have the potential to reduce anxiety. LDN has a “rebound effect” that causes the body to increase endorphin production when opioid receptors are temporarily blocked. However, research is limited and has primarily been conducted on patients with chronic health conditions. This mode of naltrexone use is not FDA-approved.
Can I take other medications with naltrexone?
Alert your physician to any medications you’re currently on or might use while taking naltrexone. Ask a medical provider before taking any medications with naltrexone.
How long after taking opioids can I take naltrexone?
You can only take naltrexone once all opioids are completely out of your system. This process can take at least seven to 10 days and may include a naloxone or urine test to confirm.
On-demand, online addiction care from home — on your terms.
Access our care team directly through an app on your phone.
At Boulder Care, we’re committed to providing clear, evidence-based information about opioid and alcohol use disorder recovery. Learn more about our editorial standards and medical review process.