{kind=link}
Language Support:
Español
中文
Tiếng Việt
한국어
Pусский
Tagalog
Українська
ភាសាខ្មែរ
日本語
አማሪኛ
Oromoo
العربي
ਪੰਜਾਬੀ
Deutsch
ລາວ
Kreyòl Ayisyen
Français
Polski
Português
Italiano
فارسی
You've got people now.
Introducing QuickStart: a naloxone-accelerated complete transition method for starting buprenorphine
On March 2nd, 2023 we hosted a webinar to share what we know about QuickStart so far — and invited questions from the community. Watch the recording below, and you can download the slides here. Please get in touch if you have questions, experiences to share or are interested in partnering with us.
The saturation of illicitly manufactured fentanyl in the U.S. drug supply has made it more challenging for people with opioid use disorder to start treatment on buprenorphine (most commonly prescribed as BUP-NX, or Suboxone), because the methods we used to use to help people start on buprenorphine are now more likely to cause painful precipitated withdrawal. This has led to an urgent call for new methods that can be individualized to each person’s unique case.
Most common alternative methods for BUP initiation focus on reducing a patient’s risk of precipitated withdrawal — but to do so, they extend the time the transition takes to complete, therefore prolonging exposure to fentanyl’s harms.

Long transition periods and the fear of unpredictable withdrawal can deter people from seeking BUP treatment and cause return to use. QuickStart offers a groundbreaking, new, and much quicker alternative.
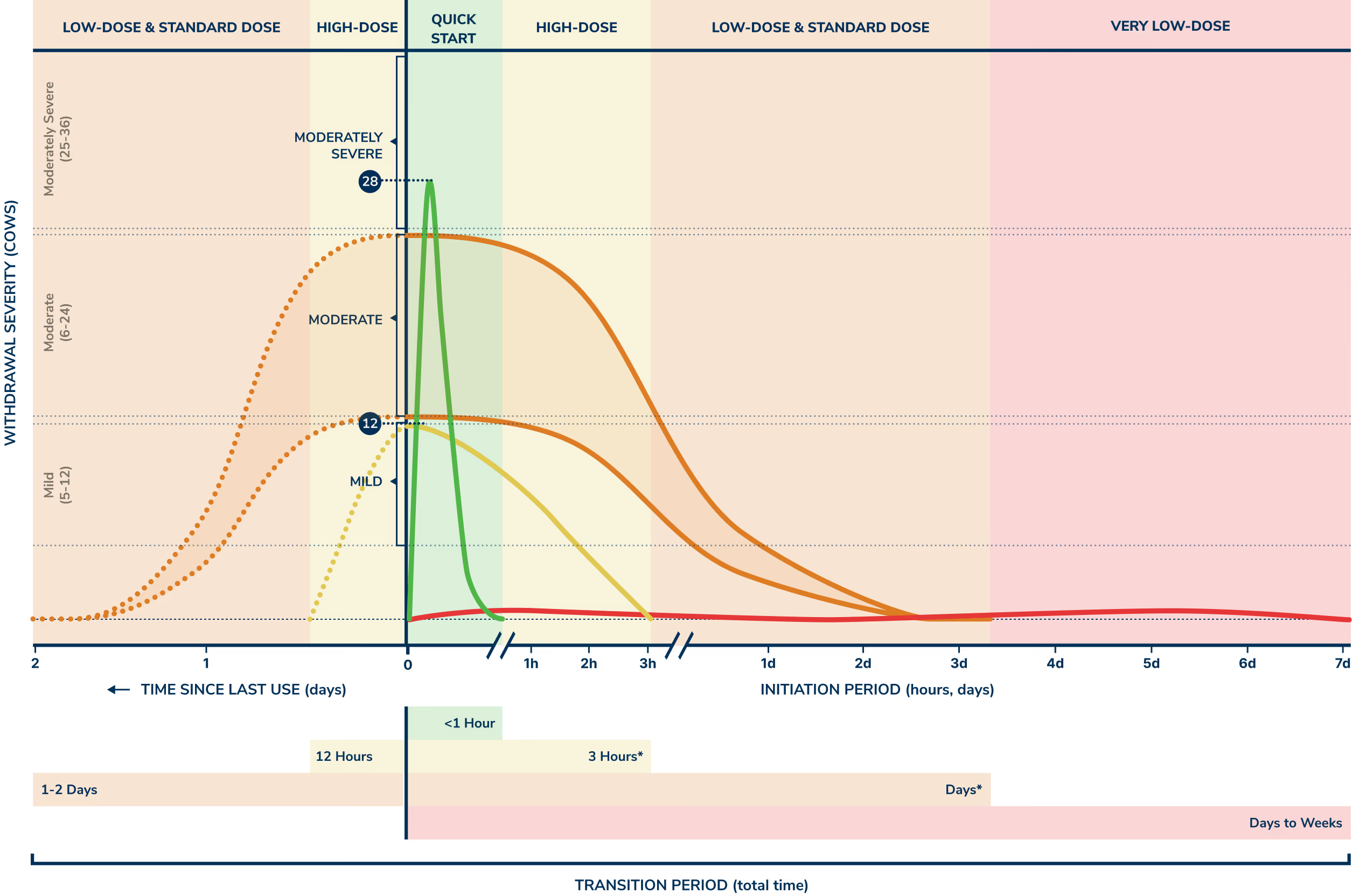
QuickStart is a new method for initiating buprenorphine-naloxone (BUP-NX), also known as Suboxone. It uses naloxone (commonly known as Narcan) to clear opioid receptors at the start of your transition from fentanyl. This eliminates the need to wait after your last use of opioids, and means you can start a full dose of BUP-NX right away, without tapering. You can prepare for a short, controlled withdrawal period that lasts only minutes, and your clinician may help prescribe medications that make symptoms more comfortable. QuickStart is intended for patients with recent use of opioids who are not yet experiencing significant withdrawal symptoms.
You can expect the full QuickStart process to take less than an hour.
Starting the moment you're ready avoids the need for severe, uncertain, and prolonged withdrawal. Waiting periods are fraught with the risk of returning to use and exposure to the lethality of fentanyl.
You can take a full dose of buprenorphine right off the bat. No need to follow a complicated tapering schedule, or continue to use fentanyl during your transition. Stop when you want, right away.
The full process is so fast, it’s measured in minutes, not days. So far, all of our patients have completed the process and felt good enough to sleep within an hour.
Yes, you will experience moderate withdrawal. But it is very short — minutes — and under your control. As soon as you start to feel symptoms, you take a full-dose of BUP-NX, which acts quickly to ease them.
This method is unique in that it relies on naloxone — not to reverse an overdose, but to clear your receptors instantly so the full dose of BUP-NX can be introduced.
You decide when and where you’re ready. You don't need to go to a clinic, and you're able to self-administer and control the entire process in a very short period of time.
If you're interested in trying QuickStart for yourself, we're here to help. See if you're eligible to enroll with Boulder.
Get StartedInterested in learning more about how to provide QuickStart to your patients or community?
Contact our team“Used nasal spray naloxone at 9:30. At 9:45 begin taking 24 mg of Suboxone. By 10:00 felt
significantly better. Thank you... I hope this method catches traction, could save a lot of lives. The experience was MUCH easier to handle than precipitated withdrawal and was over much faster than I thought it would be”
“Highly recommended. You will be sick for an hour and then you will be perfectly fine…I think [this] will save a lot of lives.”
“I just wanted to update you on how it went. I took the suboxone at about 10 minutes after taking my naloxone...After the buprenorphine dissolved and kicked in I ended up sleeping all night as well and woke up feeling fine.”
The QuickStart method starts with administering naloxone (an opioid antagonist, aka Narcan). Naloxone clears the opioids in your system, including fentanyl, from the brain’s opioid receptors. This will also start withdrawal symptoms. As soon as those symptoms begin, you'll quickly start on a full dose of BUP-NX (partial opioid agonist, aka Suboxone) to cover the newly cleared opioid receptors.
The BUP-NX limits and ends your withdrawal quickly while it also protects your receptors from any remaining fentanyl (or other full opioid agonists) in your system. Your brain and body adjust to this new, stable dose of BUP-NX. You don’t need to taper your opioid use ahead of time or after, and you don't need to slowly increase your buprenorphine dose after to get to a stable dosage level.
The QuickStart method is an emerging science, and like any method, experiences will vary from person to person. But according to patients who have tried QuickStart, you can expect 30 minutes of moderate withdrawal symptoms, and a total time of about 1 hour for the entire process. Most patients are ready for a nap after about 30 minutes, and wake up feeling symptom free and stable.
After you've completed the QuickStart method, you can continue your recovery journey in the way that works best for you, and take BUP-NX (Suboxone) regularly as prescribed.
Because QuickStart is certain to induce withdrawal for a short period, this method requires that patients are able and willing to tolerate more significant withdrawal symptoms than is expected in other methods, even if that withdrawal lasts for less time. For this reason, particular caution should be used in counseling patients with underlying cardiac disease or unstable psychiatric conditions. Some patients will feel the temporary discomfort is worth the speed at which the transition can be completed while others will not.
In times of crisis — wounds in World Wars, burns in mass casualties, and the HIV/AIDS epidemic — the medical community has had to respond in seemingly unconventional ways to save lives. People suffering from OUD are pleading for the same intrepid focus to help them begin BUP-NX.
“Rapid research, in partnership with people who use drugs and using community-based participatory research practices to ensure trust, shared goals, and an absence of adverse consequences, should be conducted to help identify the factors associated with successful and failed inductions.” –Fiellin, David A. MD
"With the worst opioid overdose death crisis in the United States history, urgent new approaches to assist people who use drugs onto medication for opioid use disorder are necessary. People who use drugs should be involved at all levels with ongoing research, clinical and policy efforts to improve buprenorphine initiation as their lives and their suffering are at stake." –Kimberly L Sue et al
If you're interested in QuickStart for yourself — Boulder patient or not — we're to help. See what your options are, and if you're eligible for Boulder.
Get StartedInterested in learning more about QuickStart and how you can partner with Boulder or provide this protocol for your patients or community?
Please don't send any medical questions or personal health information via this form. If you are a potential patient looking to get started with Boulder, please get in touch with us here
Our mission is to improve the lives of people with substance use disorders. We provide medication, resources, and support to help our patients succeed on their own terms, wherever they are.