Opioid use exists on a spectrum, and the difference between typical use, physical dependence, and opioid use disorder isn't always immediately clear.
Signs of opioid use disorder are patterns that develop over time and may affect many different areas of a person's life.
Early changes may be subtle, but paying attention to them can make it easier to take action before they become more serious.
Support can be helpful at any stage, and you don't have to wait for things to feel "bad enough" to reach out.
Opioids are a class of drugs widely used to relieve pain. These medications work exceptionally well at the right doses in hospitals, for short periods during recovery, and in hospice care. However, due to the way the body often responds to the euphoric effects of the opioid, it’s easy for problematic use patterns to develop.
Opioid use disorder (OUD) is a condition that involves cravings, loss of control, compulsive use, and continued use despite harm. Use can shift along this spectrum, making it difficult to know what’s normal and what's problematic dependence.
That uncertainty is common. Opioid use doesn't always seem severe. For many people, it often falls somewhere in a gray area where you notice greater dependence on your medication, but still feel unsure whether it's something to be concerned about.
In this article, we’ll unpack the signs of opioid addiction but will primarily use the term “opioid use disorder” for the sake of clinical accuracy.
Knowing more about the difference between typical use, physical dependence, and opioid use disorder can help you make informed decisions about your health.
Our program is based on your goals, not our rules.
Whether you want to reduce use or stop altogether, your care team has your back.
Opioid use disorder is a medical condition where someone’s pattern of opioid use becomes difficult to control and continues even after they’ve experienced the harmful consequences of addiction.
"The diagnostic criteria are less important than the lived experience they're trying to capture: I keep doing this even though I don't want to, even though it's costing me things I care about, and I can't seem to stop on my own," explains Shannon Boustead, MD, a community engagement physician at Boulder Care.
OUD can range from mild to severe, depending on the number and intensity of symptoms a person experiences. Symptoms may show up as changes in mood, behavior, and physical health. Over time, if the condition isn't treated, these signs become more serious and difficult to ignore.
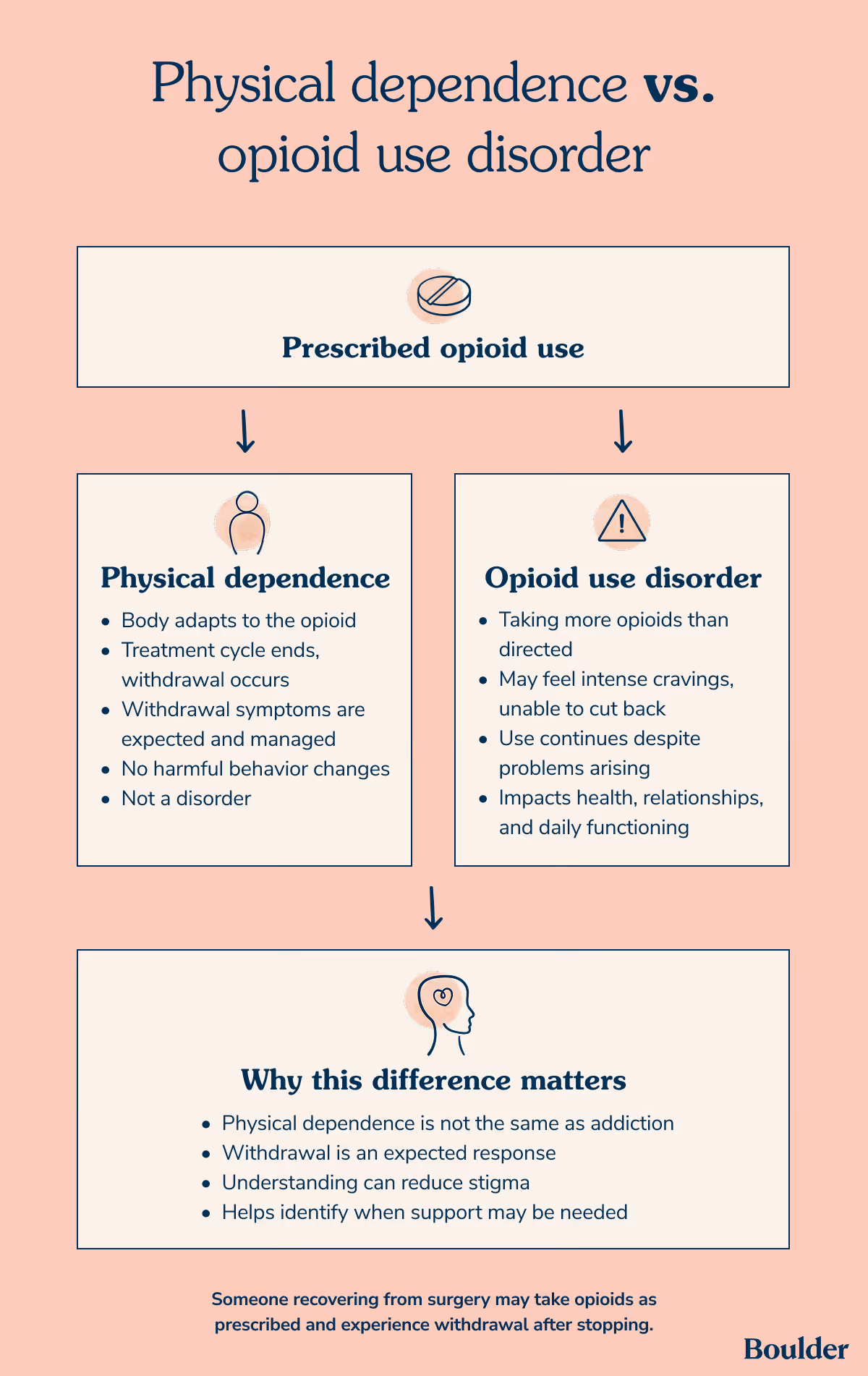
The difference between physical dependence and opioid use disorder
The difference between physical dependence and opioid use disorder is that dependence refers to the body adapting to a drug, while opioid use disorder involves a pattern of use that becomes difficult to control despite negative effects.
Physical dependence
As Dr. Boustead explains, "Physical dependence is a physiological adaptation—the body has adjusted to the presence of the drug, and stopping it causes withdrawal. That is an expected, predictable consequence of opioid exposure. It happens to patients on long-term pain therapy...It is not, by itself, a disorder."
Physical dependence can happen even when opioids are taken exactly as prescribed. For example, someone recovering from surgery might take an opioid medication to control pain for a few weeks, leading to dependence.
If they stop taking the medication, they could experience withdrawal symptoms. In this case, their body has gotten used to the medication, but they are taking it as prescribed without any harmful behavioral changes.
Opioid use disorder
Opioid use disorder, on the other hand, involves more than physical dependence. A person might start taking a medication as prescribed, but then take more than directed.
They may then feel unable to cut back and continue using opioids even when they start to have problems with their health, relationships, work, and daily functioning.
Physical dependence alone doesn’t mean someone is addicted to opioids. Withdrawal symptoms are a normal—albeit uncomfortable—response to taking opioids for some time.
Knowing this difference can help reduce some of the stigma that comes from feeling dependent on opioids, plus make it easier to recognize when more support might be needed.
Get the medication you need, and the support you deserve.
We provide FDA-approved medications for alcohol and opioid addiction — and support services to help you stay on track and reach your recovery goals.
Mental health conditions, such as depression, anxiety, or PTSD
A history of trauma or high stress
Starting opioids at a younger age
Social and environmental factors like limited support, exposure to substance use, and unstable housing
Having one or more risk factors doesn't mean that a person will develop opioid use disorder, but they can make certain patterns more likely to emerge.
Signs of opioid use disorder: Why patterns matter
Symptoms of opioid use are best understood as patterns that gradually emerge over time. This isn't a checklist you can tally up to get a score. No single sign on its own means that someone has a disorder, and you don't have to relate to every sign for something to be worth paying attention to.
How the brain works, including how it processes reward, stress, and physical discomfort, influences how these patterns progress. Dr. Boustead notes that the brain reorganizes itself around this chemical signal, lowering its natural production of feel-good neurotransmitters and adjusting what "normal" feels like.
"By the time someone notices something is off, they're already chasing a baseline that has shifted beneath them—often without any conscious awareness that the shift occurred," he says.
Early changes, such as taking a little more than intended or thinking about use more often, can be easy to explain away. You needed a little extra because your pain was worse. You're thinking about your next dose because your pain is creeping back.
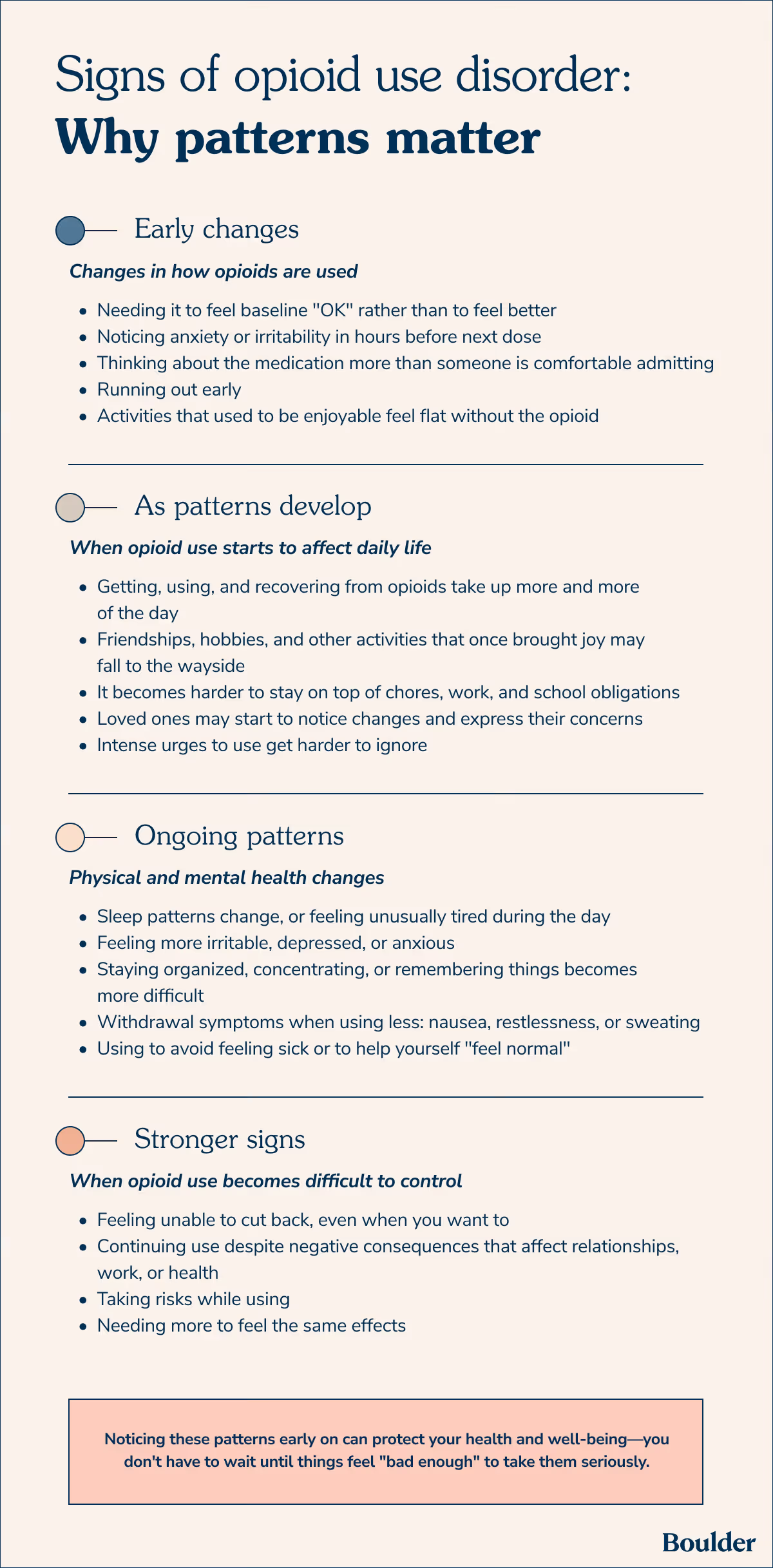
Over time, however, these patterns start to affect daily life more and more, including your physical and mental health and the ability to cut back. Noticing these patterns early on can protect your health and well-being—you don't have to wait until things feel "bad enough" to take them seriously.
"The earlier someone gets accurate information about what's happening in their body and brain, the more options they have, and the more agency they retain," Dr. Boustead says. "What gets lost when OUD goes unrecognized isn't just health—it's time, relationships, trust, and often the person's own self-understanding."
Early signs: Changes in how opioids are used
While many people are still able to keep up with work, relationships, and responsibilities, they still notice subtle changes in how opioids are used. Seeming "fine" on the surface doesn't always mean that everything feels under control.
Part of the reason why early signs are easy to miss, Dr. Boustead explains, is that the initial experience of opioids doesn't feel like a problem–it feels like a solution. "Pain relief, anxiety quieted, social ease, sleep. The brain registers this as ‘that worked.’ And it did work, at least in the short-term.”
That was Crystal Campbell's experience, a Peer recovery specialist at Boulder Care, who explains that those early changes felt like relief. "It actually felt like something was finally helping me cope. Because of that, it was really easy to explain it away and tell myself I had it under control."
He also points to the cultural narrative around addiction as a barrier to early recognition. "We've spent decades telling the public that addiction means moral failure, loss of control, hitting rock bottom. So someone who is still going to work, still paying bills, still mostly showing up—they don't see themselves in that story. And they're right that the story doesn't fit them. What they don't realize is that the story was wrong to begin with."
Dr. Boustead describes the early shift he watches for most carefully as a change in the relationship to the medication, not just the dose. Early signals include:
Needing it to feel okay rather than to feel better
Noticing anxiety or irritability in the hours before the next dose
Thinking about the medication more than feels comfortable admitting
Running out early
Finding that activities that used to be enjoyable feel flat without it
He also pays close attention to context: "Someone who started on opioids for a finite reason—post-surgical pain, an acute injury—and is still using them months later for reasons that have gotten harder to articulate: that warrants a real conversation."
As patterns develop: When opioid use starts to affect daily life
Over time, ongoing patterns of opioid use can move beyond the initial concerns and start to show up in ways that have more serious effects on a person's everyday life. This can include:
More time spent on opioids: Getting, using, and recovering from opioids start to take up increasing amounts of a person's day.
Pulling away from things that used to matter: Friendships, hobbies, and other activities that once brought joy may fall to the wayside as opioids take a more central role in a person's life.
Struggling to keep up with responsibilities: Daily functioning begins to slip, and it becomes harder to stay on top of household duties, work deadlines, and school obligations.
Tension in close relationships: Family members or friends may start to notice changes and express their concerns, which can lead to arguments and mistrust.
Stronger cravings: Intense urges to use get harder to ignore, often making it difficult to focus on anything else.
These patterns don’t emerge because a person lacks willpower or care. Opioids cause changes in the brain, which is why they can lead to opioid dependence and addiction. Noticing these changes and getting professional support can make a major difference.
Ongoing patterns: Physical and mental health changes
As you continue using opioids, the effects often start to take a more significant toll on the mind and body, which are increasingly difficult to ignore.
Mood changes: You may feel more irritable, depressed, or anxious.
Changes in focus or memory: Opioid use can affect cognition, so staying organized, concentrating, or remembering things you need to keep track of may become more difficult.
Withdrawal symptoms when use decreases: This is partly related to how long opioids stay in your system, which varies based on the type of opioid, the dose, and other factors. Short-acting opioids used for pain relief tend to wear off faster, so if you take less than normal or miss a dose, you might feel physically unwell with symptoms like nausea, restlessness, or sweating.
Using to avoid feeling sick: You might not take opioids to feel better, but to prevent withdrawal symptoms or just to help yourself "feel normal."
Stronger signs: When opioid use becomes difficult to control
Opioid use can go from feeling manageable to something that feels harder to stop, even when you want to cut back. For Campbell, this was a gradual process. "I started thinking about it more, planning around it, and noticing I didn’t feel right without it. Over time, my day started revolving around it more than I realized, and that’s when it hit me that it might be more serious than I originally thought."
This is when the pattern becomes more disruptive, which may include:
Feeling unable to cut back when you want to, but finding it harder than you thought it would.
Continuing use despite negative consequences that affect relationships, work, health, and other areas of your life.
Taking risks while using, such as combining opioids with other substances, taking them in unsafe situations, or continuing to use despite safety concerns.
Needing more to feel the same effects, since the dose you were previously taking feels less effective.
Dr. Boustead describes the clearest sign this way: "When someone is using opioids not to treat a symptom but to avoid the suffering of not having them." He explains that once a person has experienced opioid withdrawal symptoms, including symptoms like nausea, aching, insomnia, and anxiety, avoiding them becomes a powerful motivator in its own right that overrides a person’s values and commitments. “When that need has started making decisions for them—how they spend money, who they spend time with, what they're willing to risk—that's the line."
He is careful to add: "Crossing that line doesn't make someone a bad person. It makes them someone whose brain has been changed by a powerful drug, and who deserves treatment."
What to do if you recognize these signs in yourself
It’s normal to feel worried and confused if you notice these patterns in yourself, especially when some aspects of your life seem manageable while others don't.
Because opioid use exists on a spectrum, it's normal to feel like you might be somewhere in the middle. Recognizing these signs is an important step so you can decide what kind of support and changes might be right for you.
Talk to a healthcare provider: A clinician at Boulder Care can help you understand what you're experiencing and walk through your next steps.
Set small, realistic limits: Your doctor can help you figure out a tapering strategy that’s right for you. This might involve gradually reducing your dose, or you might try spacing out doses or setting clear boundaries to see how it feels.
Reach out to someone you trust: Share what you've noticed with a supportive friend, partner, or family member.
Explore support options: This might include medication-assisted treatment (MAT), counseling, support groups, and peer support. There are different options, and no single choice is the "right" one for everyone.
You don't have to have it all figured out at this point. What matters is that you're paying attention to these changes and taking steps to get the support you need.
What to do if you recognize these signs in someone you love
Noticing signs that someone is using opioids can leave you feeling worried, frustrated, or hopeless. But you're not responsible for diagnosing or solving the problem on your own. Your role is to be supportive and reduce harm where you can.
Show concern but avoid confrontation: How you communicate matters. Confrontation can backfire, often feeling more like judgment and stigma instead of concern. Mention some of the changes you've noticed without labeling or accusing.
Choose the right moment: Don't bring it up when emotions are hot or the situation is unstable. Wait for a calm, private moment to have a conversation.
Clearly express support and care: Supportive relationships can improve recovery outcomes. Let them know you're worried because you care about them, not because you are criticizing or trying to control them.
Don't argue about what it means: It's not your job to label or diagnose them; only a clinician can do that. Instead, focus on the behaviors and emotions that have changed.
Encourage support, but don't pressure: Suggest talking to a healthcare provider and suggest checking out some resources without invading their autonomy.
You can't force them to change, but you also don't have to carry your worries alone. Compassionate support can help, but it's also important to pair it with healthy boundaries that protect your well-being.
The bottom line
Spotting the signs of opioid use disorder isn't about checking boxes off a checklist or applying labels. OUD exists on a continuous spectrum. Patterns can look different from one person to the next and often change over time.
If you're recognizing some of these patterns, it doesn't mean that things have to get worse before they get better. Support looks different for everyone, and there are flexible ways to explore what can help—including medications and online support.
What are the most common signs of opioid use disorder?
Common signs of opioid use disorder include losing control over use, craving opioids, physical dependence, and behavior changes that interfere with a person's ability to function in their daily life. Only a clinician can make a diagnosis, and it's possible to feel like you need to get help even if you don't meet the diagnostic criteria for OUD.
How quickly can opioid use disorder develop?
Opioid use disorder doesn't have a set timeline. You can come physically dependence on opioids within days or weeks of repeated daily use of opioids. But that doesn't mean that you have a disorder.
The risk of developing an opioid use disorder increases the longer a person takes opioids, especially if taken for longer than 90 days. The Centers for Disease Control and Prevention (CDC) suggests that around 25% of people who take opioids long-term may eventually develop an OUD. Because of this, opioid therapy requires regular reassessment to help assess risk and check for early warning signs.
Can you be physically dependent without having opioid use disorder?
Yes, you can be physically dependent on opioids without having opioid use disorder. If you are physically dependent, it means that your body has adapted to the medication, so you'll experience symptoms of withdrawal if you stop taking it. OUD is characterized by additional symptoms such as feeling unable to cut back, taking opioids despite negative consequences, and engaging in risky behavior.
On-demand, online addiction care from home — on your terms.
Access our care team directly through an app on your phone.
At Boulder Care, we’re committed to providing clear, evidence-based information about opioid and alcohol use disorder recovery. Learn more about our editorial standards and medical review process.